Hysterectomy with and without salpingectomy or oophorectomy is considered by World Professional Association for Transgender Health to be a medically necessary part of gender affirming surgical therapy for those transgender men who choose to sought this procedure. Hysterectomies are followed by transgender people who were presumed female at birth, including men and non-binary people to stop menstruation, prevent any possibility of pregnancy, or for other health issues. Actually, not all transgenders want, sought or can have surgery, and being trans doesn’t necessary means that you should have surgery.
There are different surgical options and choosing the applicable procedure depends on several issues like: physical capacity and needs of the patients and surgeon’s expertise.
Hysterectomy surgical options include :
Abdominal laparotomy : it involves a incision in the lower abdomen
Transvaginal : it involves removing the womb through the vagina or front hole.
Abdominal laparoscopy : it involves a tiny incisionnear the navel.
Options of Hysterectomy
Also, hysterectomy consists of several options which are as follows :
Full hysterectomy
all parts of the genital organs including: uterus, cervix, fallopian tubes and ovaries will be removed.
Partial hysterectomy
the uterus and fallopian will be removed.
Oophorectomy
only ovaries will be removed.
Hysterectomy may get done abdominally, laparoscopically or vaginally. According to some evidences, the procedure through vagina has less complications like than other approaches. Also, there won’t be any abdominal scar. Hysterectomy can be combined with other transgender surgeries like vaginectomy, mastectomy and genital reconstruction. Hysterectomy itself does not largely differ, however some alternations in simultaneous surgeries and extent of dissection may differ depending on the goals of the transgender patient. For example if a transgender man undergoing hysterectomy has no plans for penetrative vaginal intercourse in the future, the vaginal cuff closure could be much more exterior, such that less of a vaginal orifice remains.
Risk Factors of Hysterectomy
Adverse reactions: Nausea and vomiting, breathing or heart problems due to anesthesia.
Pain from CO2 gas: At the beginning of surgery, your abdomen is filled with gas to give the surgeon adequate internal visibility of your organs. The CO2 gas can become trapped against the diaphragm causing organ, diaphragm and possibly shoulder pain.
Infection: Wound infection or infection of the bladder, chest, or abdomen may necessitate antibiotic treatment.
Urinary problems: Kidney, bladder and/or urinary tract infection; temporary urinary incontinence or retention, requiring continued use of a catheter.
Hemorrhage: Excessive blood loss during or after surgery which requires blood transfusion.
Blood clots: Can happen in the veins in the leg or pelvis. The risk is increased by smoking, inactivity, excess weight and oral contraceptives.
Adjacent organ perforation: Rectal fistula, vesicovaginal fistula or urethral fistula are serious complications that involve an abnormal connection between two spaces and fecal and/or urinary incontinence.
Bilateral Salpingo-Oophorectomy
as we previously discussed, in hysterectomy the uterus is surgically removed with or without other organs or tissues.
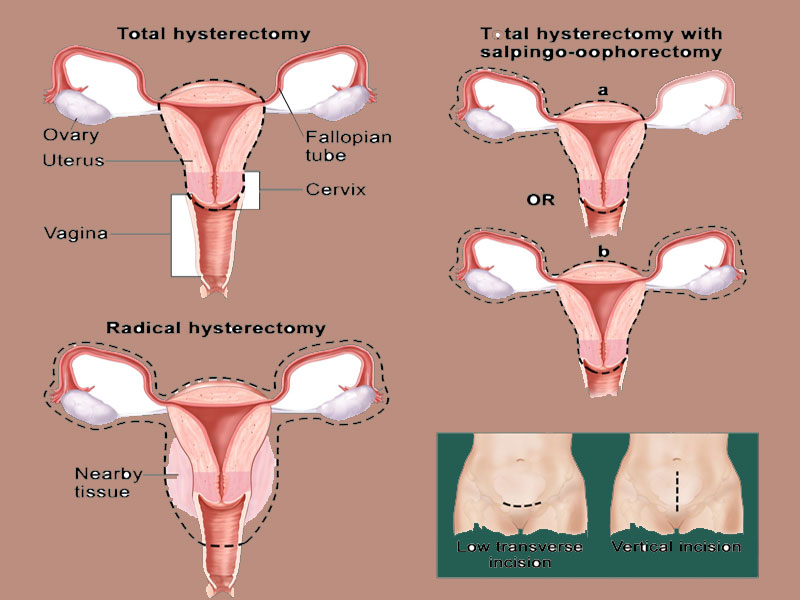
In a total hysterectomy, the uterus and cervix are removed. A total hysterectomy with salpingo-oophorectomy includes two procedures:
- the uterus plus one (unilateral) ovary and fallopian tube are removed;
- or the uterus plus both (bilateral) ovaries and fallopian tubes are removed.
In a radical hysterectomy, the uterus, cervix, both ovaries, both fallopian tubes, and nearby tissue are removed. These procedures are done using a low transverse incision or a vertical incision. A bilateral salpingo-oophorectomy is a surgery to remove both of your fallopian tubes and both of your ovaries.
After your surgery, you’ll stop menstruating (getting your period). You may have normal symptoms of menopause, including night sweats, hot flashes, and vaginal dryness. If you’re in menopause or have already gone through it, you may still notice some of these symptoms. Talk with your healthcare provider about ways to manage them.

After your surgery, you’ll stop menstruating (getting your period). You may have normal symptoms of menopause, including night sweats, hot flashes, and vaginal dryness. If you’re in menopause or have already gone through it, you may still notice some of these symptoms. Talk with your healthcare provider about ways to manage them.
This procedure can be combined with hysterectomy.In many countries, hysterectomy with salpingo-oophorectomy is a condition for legal recognition of the male sex; in addition, all transsexuals consider it extremely important for their well-being. Single-stage gender affirmation surgery is performed by a team of gynecology specialists and gender surgeons. The approach begins with hysterectomy and proceeds with metoidioplasty or total phalloplasty at the same stage. When bilateral mastectomy is planned, it is performed at the same time as transvaginal hysterectomy or, if laparoscopic hysterectomy is used, simultaneously with metoidioplasty. Indications for laparoscopic approach include patients’ preference and nonobese persons. After uterine vessels are identified on each side and clamped, uterine fundus is delivered posteriorly to identify, cut, and suture-ligate uteroovarian ligaments. Infundibulopelvic ligament is clamped and suture-tied, and adnexa are removed.
Risk Factors of Bilateral Salpingo-Oophorectomy
- Pain
- Infections occur in 10% of the patients.
- Anesthesia-related problems such as rapid breathing
- Fatigue
- Headaches
- Hair loss
- Palpitations
- Hot flashes
- Insomnia
- Joint pain
